Abdomen and Bleeding from the Gut – By Dr. Gnana Sankaralingam
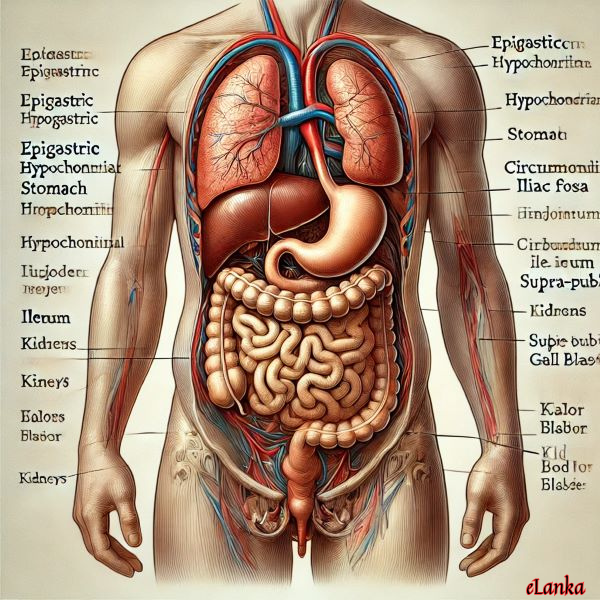
 Abdomen is bounded above by chest separated by diaphragm, a muscular dome shaped structure and below by pelvic muscle floor. Diaphragm supplied by phrenic nerves is vital for breathing, and transection of spinal cord in neck injury above sixth cervical vertebra will end in death. On the front surface, abdomen is marked into regions: Epigastric which is just below the end of breast bone (Sternum), hypogasgtric above navel, hypochondrium on both sides below rib cage, liver in right segment and spleen in left. Stomach and Pancreas lie in hypogastrium. Around the navel is called circumumbilical, which is important as referred pain from small intestine is felt there. Iliac fossa is on both sides above pelvis, with appendix being on right and lower colon on left. Area above pelvis at the middle is supra-pubic where the bladder is, and under rib cage in both flanks are loins, where the kidneys are.
Abdomen is bounded above by chest separated by diaphragm, a muscular dome shaped structure and below by pelvic muscle floor. Diaphragm supplied by phrenic nerves is vital for breathing, and transection of spinal cord in neck injury above sixth cervical vertebra will end in death. On the front surface, abdomen is marked into regions: Epigastric which is just below the end of breast bone (Sternum), hypogasgtric above navel, hypochondrium on both sides below rib cage, liver in right segment and spleen in left. Stomach and Pancreas lie in hypogastrium. Around the navel is called circumumbilical, which is important as referred pain from small intestine is felt there. Iliac fossa is on both sides above pelvis, with appendix being on right and lower colon on left. Area above pelvis at the middle is supra-pubic where the bladder is, and under rib cage in both flanks are loins, where the kidneys are.
Gut consisting of Stomach and intestines starting from mouth to anus is passage for food. Stomach is large pouch for receiving swallowed food, where it is mixed with juices, churned and poured into small intestines. It takes six hours for complete emptying. There it is acted on by bile from liver and juice from pancreas and digested. Remains are pushed into large intestines where mainly water is absorbed, and in the rectum they are formed as solid columns to be excreted out. Though gut is continuous tube in life, it starts as three different parts in embryo and merge into one later. Intestines are sectioned into duodenum, jejunum, Ileum, colon and rectum. Duodenum receives ducts from liver and pancreas. Blood supply to gut come from two different sources and where the two meet at upper end of stomach and lower part of rectum, can be centres for bleeds as in oesophageal varices and haemorrhoids. Gut moves in wave form called peristalsis which makes the food to pass through.
When solids or liquids are taken inside mouth, they are swallowed by voluntary actions of tongue and muscles of upper throat (pharynx) into gullet (oesophagus), and then descend into stomach by relaxation of muscular rings called cardia, at the junction between oesophagus and stomach. Digestive process begins in the mouth itself by enzymes in saliva. Difficulty in swallowing is called dysphagia, due to causes in the gullet. Blockages by foreign objects such as bones and dentures is common at narrower spots in the gullet, which are at the bottom of the neck (cricoid cartilage), mid way under arch of aorta and at the entry into stomach. Strangely, patient is able to point exactly where the block is. It may also be caused by cancer of oesophagus, where as the outer covering is lean, tumour grows more towards externally than towards internally, such that when it blocks causing dysphagia, growth had spread far outside, making prognosis poor. In stroke and Parkinson’s, dysphagia occurs due to neuro-muscular weakness, associated with drooling and choking. Ingestion of corrosives leads to stricture (narrowing) causing difficulty, which need repeated dilatations.
Stomach is divided into fundus, body and pylorus. Food in stomach is prevented from regurgitation by contraction of cardia, while food is kept in it during digestive process by muscles of pylorus forming sphincter (valve). Vomiting is forced action to expel stomach contents, either due to irritation of the lining of stomach by toxic substances or initiated by vomiting center in the brain as in head injury. To let out the vomitus, stomach contracts and cardia relaxes. Stomach could be the site of ulcers and cancerous growth. Veins at lower end of oesophagus and upper end of stomach become distended in cirrhosis of liver.

Bleeding could occur in any part of the gut, and the point of exit of the lost blood depends on the site and extent of bleeding. If large amounts are lost from the upper parts, it comes out as vomiting, while if small amounts are lost in upper parts or any amounts of loss from other parts, comes out through rectum. Vomiting of blood (haematemesis) result from ulcers in stomach or duodenum, cancer of stomach or distended veins in lower oesophagus or upper stomach. Bleeding through rectum could be frank blood from lower parts of colon or blackish blood (melena) from upper parts of colon. Sometimes blood will not be visible to naked eye as it gets mixed with stools (occult blood). These people will present as anaemia, and in all elderly anaemic patients, stools should be checked for any blood. Passing of blood per rectum may be due to cancer of large bowel, haemorrhoids (distended veins in rectum), ulcerative colitis (type of inflammatory bowel disease) and chronic diverticulitis (inflammed finger like projection in wall of large bowel). Polyps in the tract could also bleed.
Cancer of large bowels could present with vague symptoms such as weight loss, lower abdominal pain or importantly change of bowel habit. One normally constipated gets loose motions or one with normal motions gets constipated, he must seek medical opinion. Elderly must be screened regularly with stools for occult blood test. Cancer of stomach can be either a growth or an ulcer. They are often noticed in the advanced stages. They present with bloating, upper abdominal pain, indigestion, difficulty in swallowing, loss of apetite or loss of weight. Small bowel growths such as lymphomas and carcinoids are rare.
Liver, Gall bladder and Pancreas form part of digestive tract. Gall bladder acts as reservoir for bile, which could be the site of stones which may remain within it or pass down and block the passage of bile causing jaundice. When body tries to expel the blocking stone, it causes colicky pain similar to that in kidney stones. Cancerous growths can occur in biliary ducts, gall bladder and pancreas. They present with jaundice due to obstruction of bile duct, which results in pale stools. Liver cancer presents as right hypochondrial pain and jaundice. Liver can be site for secondary cancerous deposits from other parts of the body.
More Read

Fibre-optic endoscopy is the gold standard in diagnosis of gut problems. It could be oesophago-gastro-duodenoscopy (OGD) for upper parts and colonoscopy for lower parts. Endoscopes are used to view growths to take sample for testing, removal of foreign bodies, cauterising (burning) to stop bleeding, banding of veins in varices and haemorrhoids and to extract stones in bile duct. Most of the growths in colon can be removed using colonoscopy. In cancerous growths, segment of colon adjacent to it is removed. There is sphinctre (valve) in mid rectum which prevents incontinence of stools. If the cancer is above it, resection and anastomosis (joining up) is done, but if the cancer is below it, then removal of growth would result in leakage of stools, and due to that these patients need colostomy, where lower end of bowel is closed and upper end is brought out to drain into a bag worn ouside.